If you’ve ever tried to fire up your quads post-ACL surgery and felt like they ghosted you—welcome to the maddening world of arthrogenic muscle inhibition, or AMI. It’s the physiological equivalent of your quad saying, “Yeah nah,” and slamming the door shut just when you need it most.
What Is AMI?
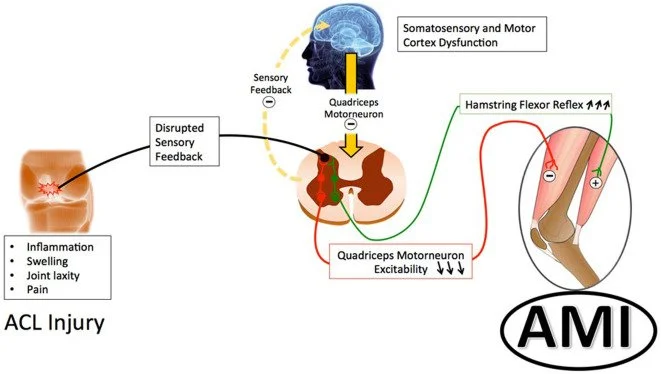
In simple terms, AMI is your nervous system throwing a protective tantrum. Following trauma (like an ACL tear or surgery), your body tries to “help” by reflexively downregulating your ability to contract certain muscles—especially your vastus medialis oblique (VMO). The end result? A limp, a loss of quad strength, and a squat that feels like it’s being powered by soggy spaghetti noodles.
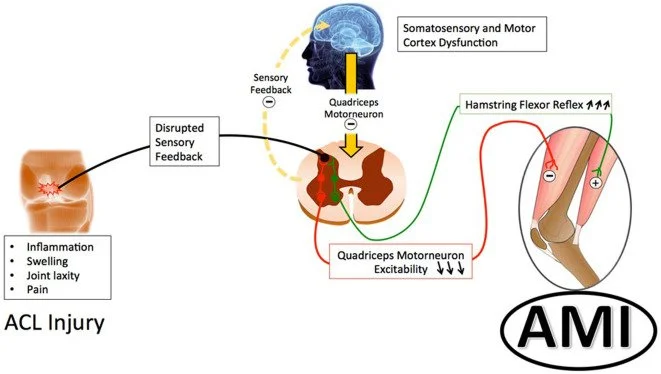
It’s not just about weak muscles—AMI is a central nervous system issue. We’re talking reflexes at the spinal level and even changes in how the brain processes movement. Imagine your quad being stuck in airplane mode.
How is it Graded & Why Should We Care?
It is more common the most people think with up to 55% of people post-ACL injury show some signs of AMI.
So hows it graded?
Grade 0:
Normal VMO activation and knee extension.
Grade 1a:
VMO isn’t firing properly, but function can return with basic exercises.
Grade 1b:
VMO activation needs more targeted and longer-term rehab to improve.
Grade 2a:
VMO is inhibited and there’s some knee extension loss due to tight hamstrings—both are reversible with simple exercises.
Grade 2b:
Similar to 2a, but doesn’t respond to basic exercises—needs longer, more specific rehab.
Grade 3:
Chronic loss of knee extension that won’t improve without surgical intervention.
Left unchecked, AMI is a one-way ticket to:
-
Loss of knee extension (which makes things like walking, climbing stairs, or showing off your lunge form a nightmare)
-
Increased risk of reinjury
-
Delayed return to sport
-
Longer-term issues
How Do We Fix It?
This is where things get interesting. Traditional tools like “cushion crush” quad sets (you know, squeezing a towel under your knee) aren’t always effective on their own. Why? Because this issue is often multifaceted and can be complex.
So what works?
Here’s what we know helps based on current evidence:
-
Cryotherapy & joint aspiration: Reduces inflammation and joint effusion that can alter proprioception in the area.
-
Neuromotor reprogramming (NR): A less common approach mixes motor imagery, proprioception, and low-frequency sound—essentially retraining the brain to stop being overprotective. Studies have shown one session can lead to a 45% improvement in VMO activation!
-
Isometric work at mid-range: Think 110% effort at specific joint angles. Iso’s can significantly help with both neuromuscular control and tendon health.
-
Neuromuscular electronic stimulation: Especially early post-op, electrical impulses to stimulate nerves and cause muscle contractions. Helps to retrain muscle recruitment pathways to “wake up” the quad.
-
Coaching: Teaching quality movement patterns and improved muscle recruitment, is key.
If you or someone you know is post-ACL and feeling like their quad’s on permanent vacation, let’s chat. We’ll help bring it back online.
